

Sex after Pelvic Pain
/Sex after pelvic pain is f*#&ing scary (no pun intended).
My lady bits, which were supposed to be my body’s Pleasure HQ, had been through hell. Over the previous decade, I’d experienced pelvic pain – specifically vulvar, vaginal, and clitoral pain – to a degree that I couldn’t use tampons, wear pants or underwear, or even walk. I was wheelchair-bound in loose maxi skirts. Needless to say, I wasn’t knocking boots much during those years.
Fast forward through the early years of pain, and meet me in my second pelvic floor physical therapist’s office. After nerve blocks and dry needles and brutal skin-rolling, my PT thought I was ready to have sex again. At the time, I was engaged and planning my wedding, and my PT and I were deep in strategy sessions for Operation: Have Sex on Honeymoon. Fortunately, she had a plan. If I prepared properly for sex, it would be possible.
How to have the most ludacris, un-romantic sex of your life.
The sex that my PT proposed was not sexy.
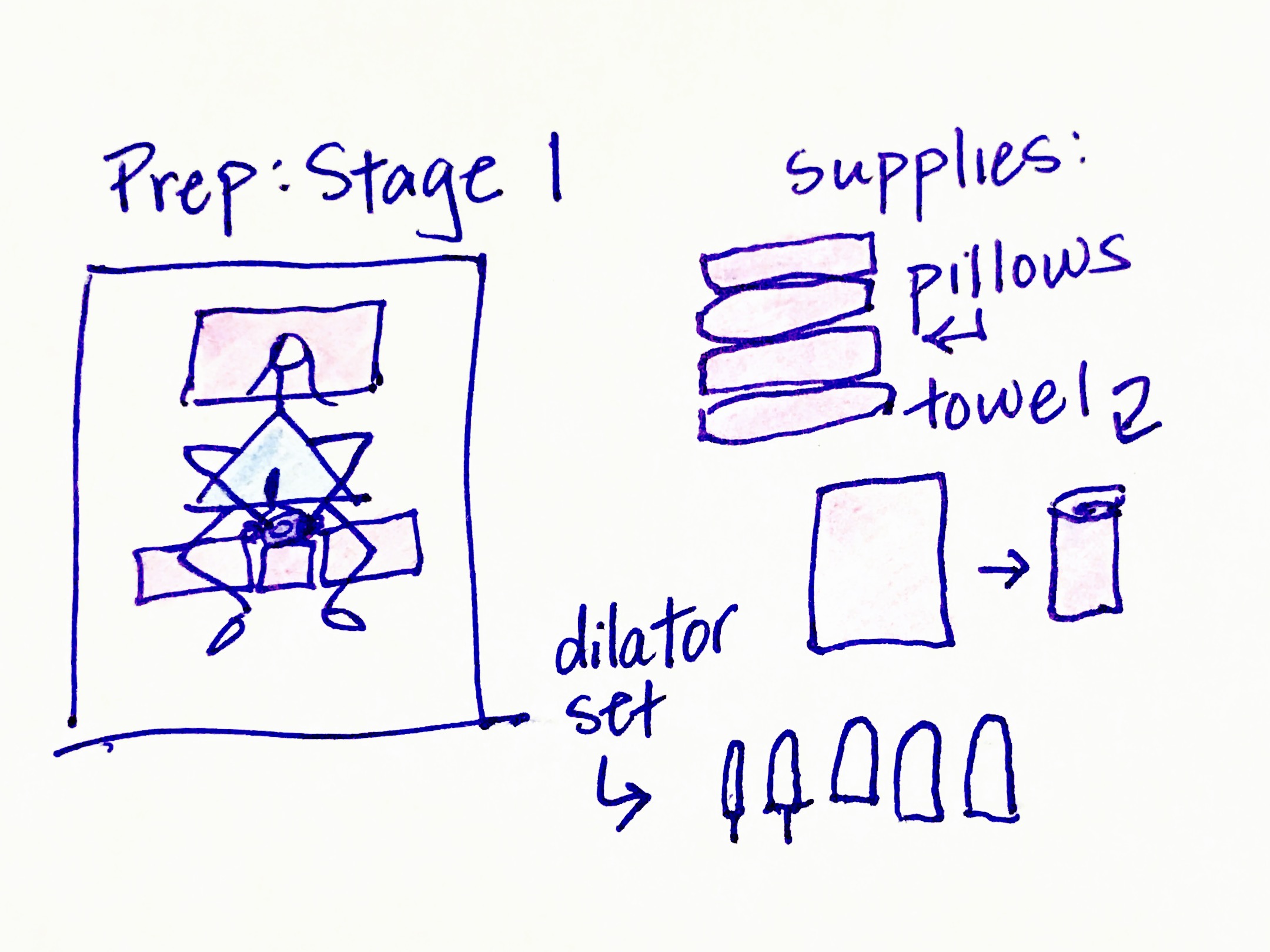
Prep Step 1: Stretch Pelvic Floor Muscles.
First, I would need to get out my set of vaginal dilators – hard, cold plastic dilators from a medical supply company. My vaginal muscles were so tight that they would literally shoot the dilators right out of my vagina upon insertion. No joke. So, I was to start with the smallest one (about the size of my pointer finger), and working up to the penis-sized one, I was to leave each of the five dilators in my vagina for about 3 to 5 minutes. To keep them from shooting out of my vagina, I was to roll up a towel and put it at my vaginal opening while I lay in a “constructive rest” position (knees bent on pillows). I then needed to stack additional pillows behind the towel to force the dilator to stay put.
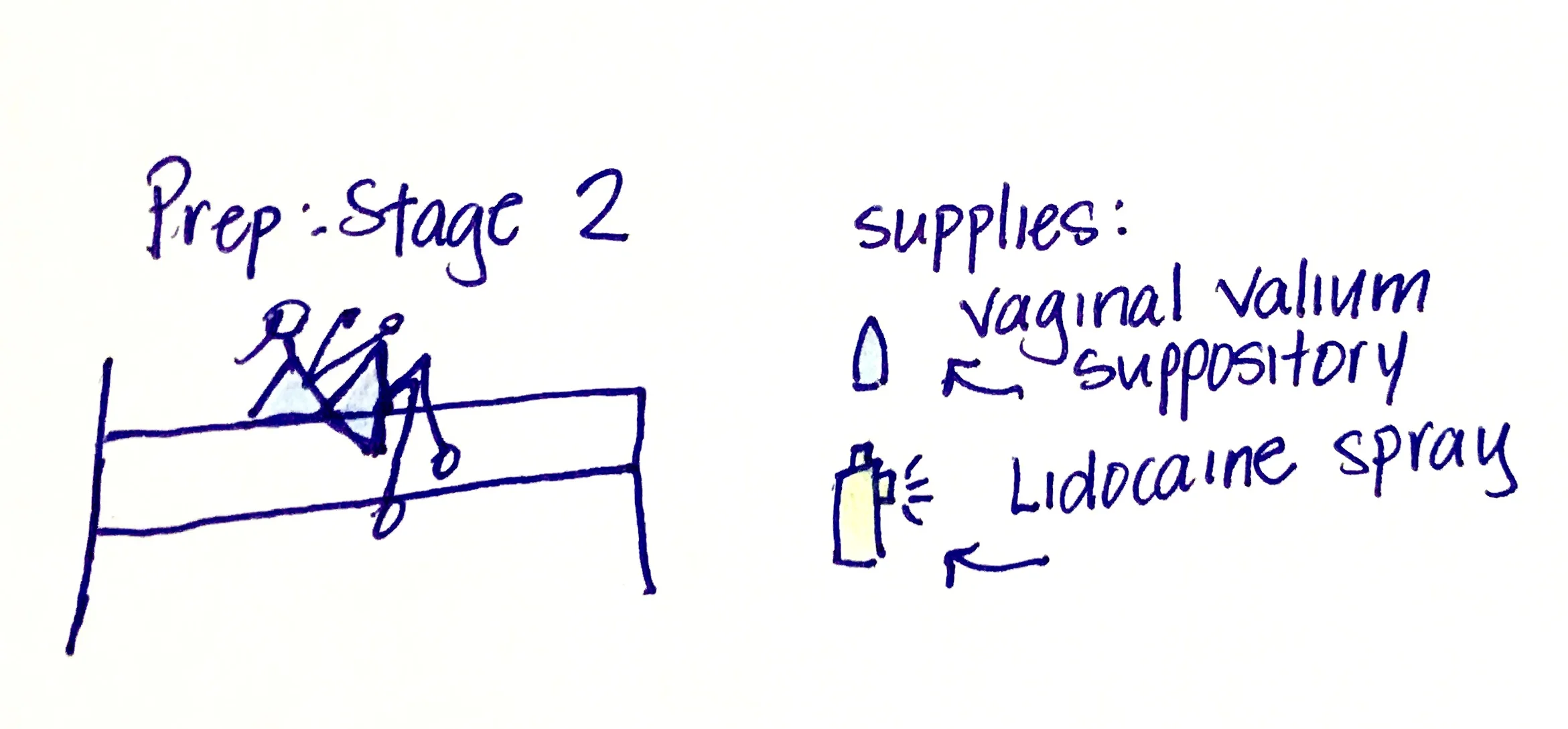
Prep Step 2: Medications.

Once the dilator exercise was done, I entered the medication phase. I started by inserting a Valium vaginal suppository. They were neon blue, dyed this crazy color by my pharmacist to distinguish the 10mg dose from the smaller doses. (No matter how much I begged them to stop using dye, they refused). After inserting the suppository, I got out my Lidocaine spray. Truthfully, it was a bottle of penis erection-prolonging spray. I sprayed it over my entire vulva, and it stung like hell. The stinging mostly stopped once the area was numbed, although only the skin numbed – the underlying soreness and pains remained.
Prep Step 3: Prepare bed.

See, I was still bleeding and tearing during sex. My perineal tissues were tender and raw, and they tore with gazillions of little papercut-looking cuts each time I used the dilators or had sex. Sex typically provoked lots of crime-scene-esque bleeding too. So, the room had to be prepared while my medications started working. I started by putting a dark towel over the bed to absorb (and hide) the blood, and then I situated the pillows where my PT had instructed me to keep my legs.
Prep Step 4: Find boyfriend/fiancé/husband.

This was actually a two-part step, and it wasn’t one addressed by my PT. But it was one that I found to be important. Turns out, after 30+ minutes of really unsexy and medicalized preparation for sex, my boyfriend/fiancé/husband often got the wrong idea. He often thought that I couldn’t possibly be interested in having sex and either (a) was working on his laptop, (b) was watching TV, or (c) was asleep. Thus, I had to locate him, convince him I was ready for sexy time, and lure him back to bed before my medications wore off.
Whew! Time for sex!
Well, sex would start with me positioning myself on the pillows just so. I’d been instructed to put my knees at 45-degree angles on pillows, keep a single pillow under my head, and remain on my back at all times. Needless to say, the time we spent actually having sex was kind of weird. Not because we didn’t have sexual chemistry and love each other and find each other sexy, but because THIS IS NOT NORMAL. It felt stilted, it didn’t feel like us, and it was a really intense reminder of how dysfunctional my lady bits and our sex life had become.
Fast-forward another three years.
My pain became worse in the intervening years, and then I moved to Chicago and met a glorious physical therapist named Sandy Hilton. Sandy had crazy ideas: sex is supposed to be pleasurable and fun and spontaneous. (Say whaaaa?!). Sandy didn’t like regimented deadlines or holding me to stilted rules. Once I was healthy enough to try sex again, she encouraged me to just “do what feels good.”
So, what did sex look like under Sandy’s rules?
Just one step:

Okay, so it wasn't quite that simple -- but almost! Before arriving on Sandy's doorstep, I had years of pelvic physical therapy, massage therapy, medications, and doctors. Nothing had helped, and nothing had made sex any less painful. And then I met Sandy, who treated me with compassion, listened intently, and educated me about pain. She didn't encourage me to return to sex until I was no longer in pain, knowing that more painful sex would just freak out me (and my trusty ol' nervous system) all over again.
Sandy told me to "do what feels good," and we had many laughs over the fact that there isn't a great graded-exposure approach for sex. So, I was encouraged to start slowly and set reasonable expectations, but no additional parameters were imposed upon sexy time. No positions or times of day or days of the month were "right" or "better." Sandy said to roll with it a little (stop the dilator-medicine-pillow routine) and throw out the dilators (go to the sex shop and get a vibrator instead -- it'll serve the same purpose but can be used for fun too, and it's not a medical device from a medical catalog). When I asked how I should "prep" for sex, she came up with "exercises" like straddling a large exercise ball and... actively straddling it to get the tissues acclimated to contact -- or a makeout session with my hubs.
There are lots of women for whom sex is painful, and it's important to note that I recovered from pain before I tackled the challenge of sex. For those in pain, sex is an immense physical and emotional challenge, and I think that the underlying issue needs to be addressed before trying to have sex (having more painful sex just compounds the problem). But once I was better, Sandy still had hard work ahead of her: convince me that I can have pain-free, enjoyable sex. Now, of course, I'm entirely delighted at how right she was!
The lesson
Sex shouldn’t be scary or painful, and often, over-medicalizing the entire process makes it even harder to return to spontaneous, fun, pleasurable sex. Sandy’s right – sex should feel good. If things don’t feel good for your lady bits, then you should ask somebody – your gynecologist or a pelvic PT – for help or insight. It doesn’t mean there’s something wrong with you, but it also doesn’t mean that you should do things that are (to quote Sandy) “anti-helpful.”
My former PT’s “sex plan” was anti-helpful. It was exhausting and uncomfortable and stilted. It made sex feel like part of a home exercise program for PT, rather than a way for me to have fun and connect with my partner. And it also made it much, much harder for me to return to sex without fear when I did finally make a full recovery.
“I somehow DID find the courage to hop back in the sack, and I’m really glad that I did. ”
Nevertheless, I somehow DID find the courage to hop back in the sack, and I’m really glad that I did. This time, it didn’t feel like my PT’s voice was in my head the whole time, narrating where my knee should go, whether my pillow was at the right height, and whether I should reapply my Lidocaine. Instead, I was able to be present in the moment. And, when I saw my pelvic pain doctor for a regular check-up the following week, I proudly reported to him: “I had sex twice last Saturday!” And he, of course, responded: “Awesome! That’s normal for a 31 year-old woman!” (he also, of course, high-fived me).
Sex is fun. If you’re not having it because of pain, get help!



